A Public Health Definition:
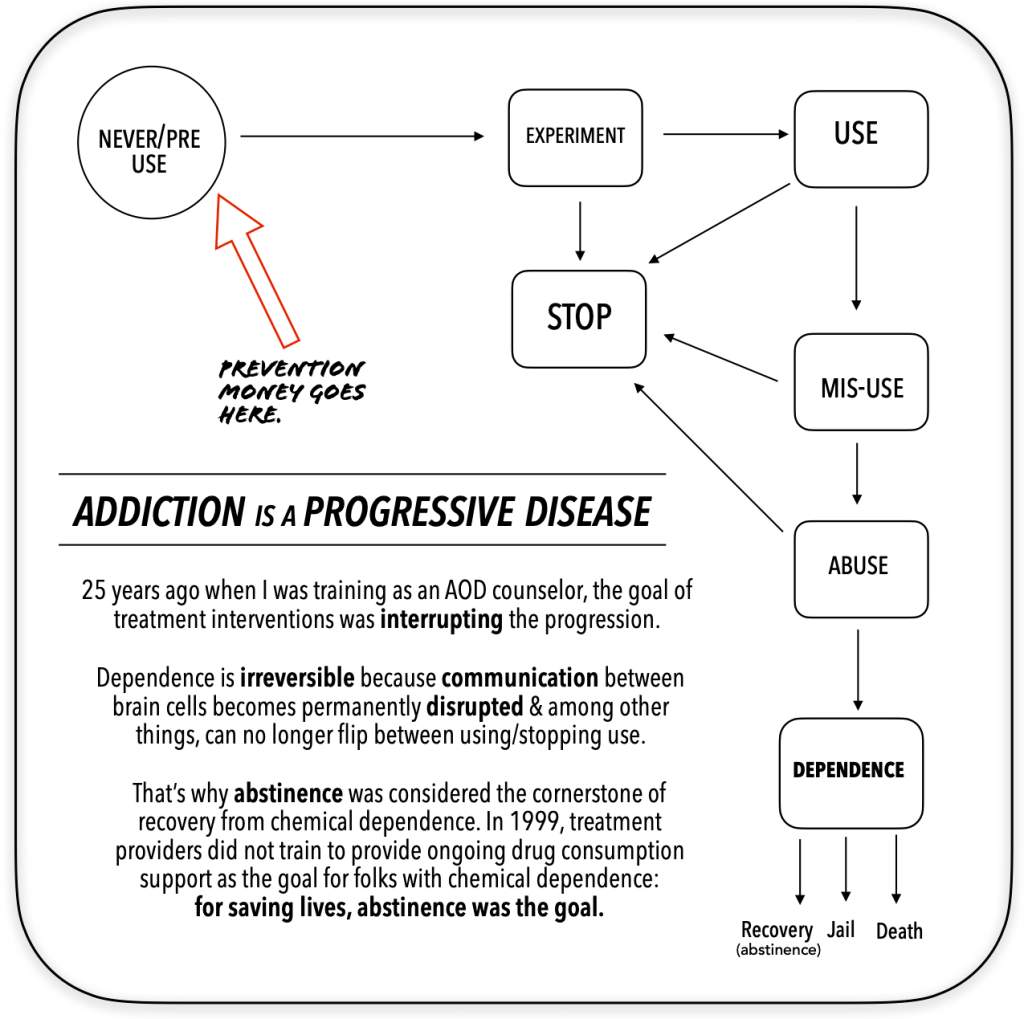
- The disease of addiction is a chronic, progressive, relapsing, incurable and potentially fatal condition with genetic, psychosocial and environmental factors influencing its development and manifestation;
- The disease is set intro motion by experimentation with the drug by a susceptible host in an environment that is conductive to alcohol & other drug misuse;
- The susceptible user quickly experiences a compulsion to use, a loss of control and will continue to use despite adverse physical, emotional or life consequences.
The clinical approach, based on this concept, is to assist the addicted individual to accept responsibility for their disease and to adopt a program of recovery with a goal of lifelong abstinence.
the American Society of Addiction Medicine and the National Council on Alcoholism and Drug Dependence. Foundations in behavioral pharmacology For Social Workers, Psychologists, Therapists and Counselors. Dr. Mark Stanford. 1998
This underpinned the entire Alcohol and Drug Abuse Counseling certification program at U.C. Berkeley Extension in 1999.
Becoming Addicted is a series of steps that can be slowed down or accelerated by public policy.
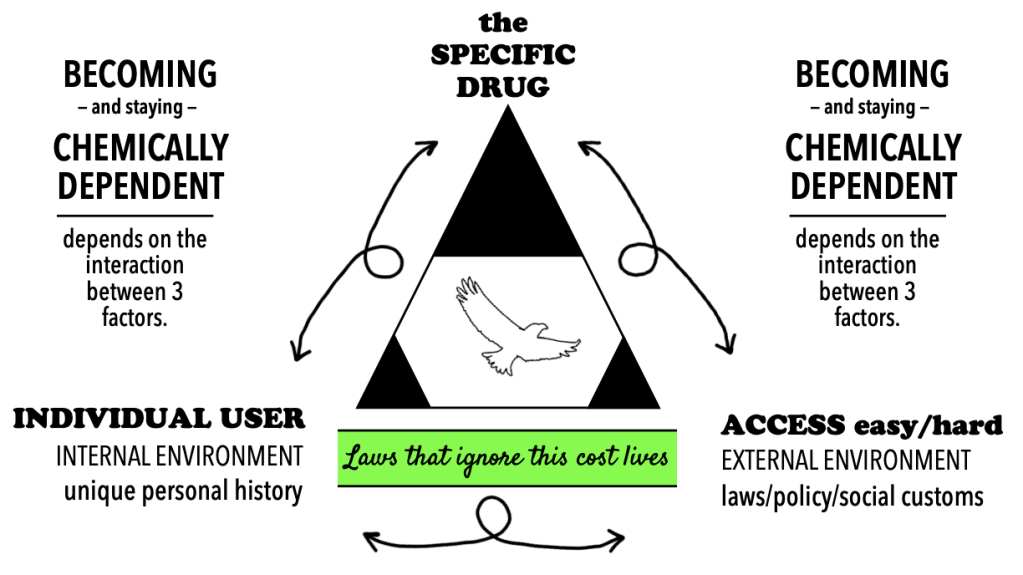
Addiction is a process enabled by intersecting circumstances. While there are as many reasons why addiction occurs as there are individual users, there are commonalities when it comes to the actual chemicals and the circumstances around how it easy or challenging it is for people to find and use them.
More drugs used by more people in more locations means more addiction.
We must consider how public policy affects ACCESS to drugs. Do legislative commitments favor increasing or decreasing access to drugs?
We should consider how public perception contributes to more or less opportunities for drug use. Do the political beliefs of community members encourage or discourage using street drugs?
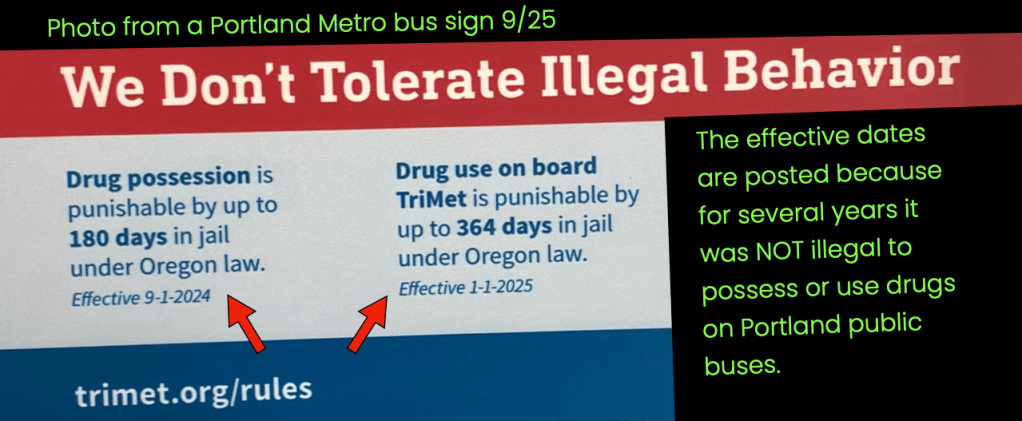
We should consider the physical locations that give people the opportunity to engage in drug use. Where is it ok to consume drugs? In Portland, This question is not hypothetical.
How Drugs Work in Our Brain:
All behavior is contingent upon the effectiveness of one brain cell communicating with another. We have about 100 billion of them that use chemical messengers called neurotransmitters to talk to each other. Behavior is a result of this communication. Because drugs are chemically similar to chemicals that already exist in the brain, they can act as a Trojan Horse and disrupt the brain cell communication system.
In order to affect the brain, a drug must be absorbed into the bloodstream and carried to the nervous system. The method of administration of a drug determines the rapidity of its absorption. Once the substance is absorbed into the bloodstream it is carried everywhere the circulatory system goes. The frequency of drug administration determines the rapidity of tolerance and withdrawal symptoms, if any.
In the brain, psychoactive drugs penetrate the blood-brain barrier and disrupt the communication of brain cells. It’s this communication disruption that changes people’s behaviors by affecting thought process and/or mood, which alters how a person thinks, feels and moves.
Behavioral homeostasis is a person’s maximum capacity defined by their genetics and environment. Our brains want to find the sweet spot not just to be more personally effective, but also for the continuation of humanity. Keeping one’s brain on an even keel means not drowning. Addicted folks are still the same people, but with their brain adapted to maintain homeostasis.
Homeostasis is maintained by dynamics that take place in the gap between nerve cells called the synapse. All psychoactive drugs work by interfering with the brain cell’s synaptic defenses. The 4 synaptic defenses are the “master pharmacists within” that help the brain maintain homeostasis. The synaptic defenses are: binding, reuptake, enzymatic degradation, autoreceptor function.
Cocaine vs. Methamphetamine: Toxicity Comp.
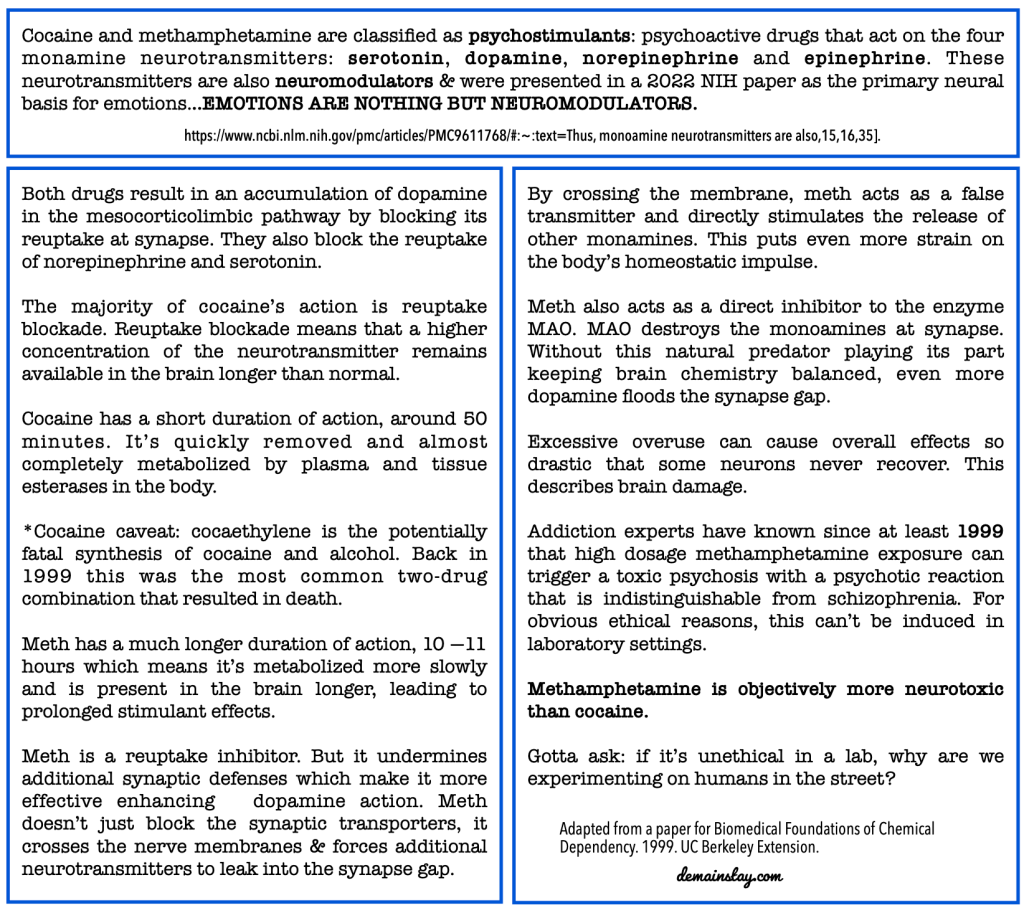
Drugs themselves reinforce their continued use through direct action on nerve cells in the brain. This direct action depletes the natural substances in the brain and so the user requires more drugs to replace them. Repeated administration of all drugs of abuse is associated with neuroadaptive responses in the brain’s reward system.
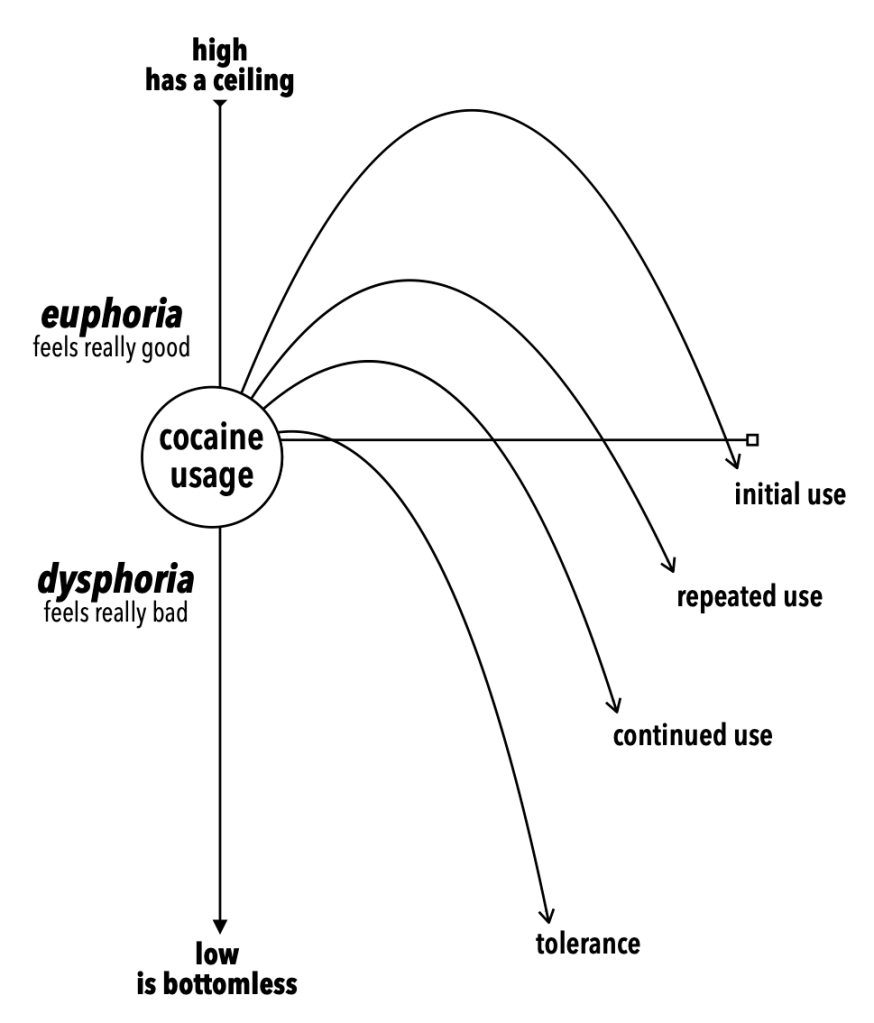
Cocaine is a stimulant that affects the pleasure center of the brain. As the brain adapts to the stimulation, it requires more of the drug to avoid crashing. At this point, the user isn’t getting HIGH but requires the drug to stave off dysphoria. As with all drugs of abuse, the pleasure ceiling has a limit & the lows are bottomless.
The brain’s reward system teaches us as a species what to do again and again for survival. Natural rewards for the brain’s pleasure circuitry include: FOOD, WATER, SEX & NURTURING. Chemical messengers in psychoactive drugs trigger the same pleasure circuitry. There is no moral hierarchy.
When the reward system is lit up, The brain feels pleasure. it can’t discern between a mother’s embrace or a dose of heroin. It’s our customs, attitudes and beliefs that inform our brain that there is — in fact — a difference between feeling good because you are being held by someone who is nurturing you and feeling good because the pleasure center in your brain’s been overrun by chemical compounds.
Due to a federal court order, where their product is sold, cigarette manufacturers must state: “when you smoke, the nicotine actually changes the brain–that’s why quitting is so hard“. same for drugs and alcohol.
Not all use is abuse! But but but
There are off-ramps from full-blown addiction if the user hits pause before tolerance sets in. Someone who does blow infrequently is not going to become chemically dependent on it.
Once the brain becomes chemically dependent, however, reverting back to casual using is no longer on the table. There certainly are prominent former addicts who are “clean” but can tolerate alcohol socially and don’t find community in the 12-step modality.
But abstinence-based treatment is an integral tool for many people to start and maintain sobriety. It was the standard of care in addiction medicine before the pivot to harm reduction in the 2000s.
Street drugs available now and in the future are designed to interrupt homeostasis unlike anything the human brain has ever known.
If, when contact was made with risky users, they were pointed AWAY from deepening their tolerance — not given the tools to encourage it — we might see different results in places experiencing drug policy failure.
Drug treatment should include abstinence-based addiction medicine.

I recently watched Brené Brown’s 2010 TED Talk on vulnerability. When she said this, at minute 17, bingo: